

Thoughts about SLPs, AAC, and FC/S2C/RPM (but mostly AAC)
I recently came across a 2024 article titled “The confidence and competence of speech language pathologists in augmentative and alternative communication: a scoping review” by Clancy Conlon, Barbra Zupan, and Robyn Preston. The article, most likely, caught my attention because of some rather conspiratorial comments regarding SLPs from proponents of Facilitated Communication (FC), Spelling to Communicate (S2C) and Rapid Prompting Method (RPM) that recently came across our social media feeds. It seems that at least some proponents believe SLPs are not only corrupt but are determined to prevent non-speaking and minimally speaking individuals from accessing spelling as a form of communication. (Not true. As this statement opposing FC/RPM explains, spelling has long been recognized as a legitimate form of communication, if appropriately feature-matched to the individual requiring AAC).

An early mechanical hand support featured in a 1998 study by Edelson, Rimland, Berger, & Billings (see recommended reading below)
FC/S2C/RPM are not, however, recognized as a legitimate form of AAC, largely because of concerns about facilitator cueing and control over letter selection, lack of scientific evidence, prompt dependency, and potential harms such as false allegations of abuse. (See Opposition Statements)
According to ASHA’s website, an ad hoc committee conducted a systematic review of FC/S2C/RPM in 2018, after which ASHA not only renewed its position opposing FC (which had been in place since 1995) but added an opposition statement that included S2C and RPM. In addition to conducting a comprehensive literature review (which revealed no evidence to support FC, S2C or RPM—see recommended reading below), committee members put out a call for public feedback about the techniques. According to the website, more than 95% of the SLPs and audiologists who provided feedback about the techniques agreed with ASHA’s decision to oppose the use of these facilitator-dependent techniques. Perhaps this is why SLPs receive such vitriol from FC/S2C/RPM proponents who claim the systematic review process was somehow “rigged.” I’m leaving that discussion for another day, but I will provide links to ASHA’s comments on this topic below.
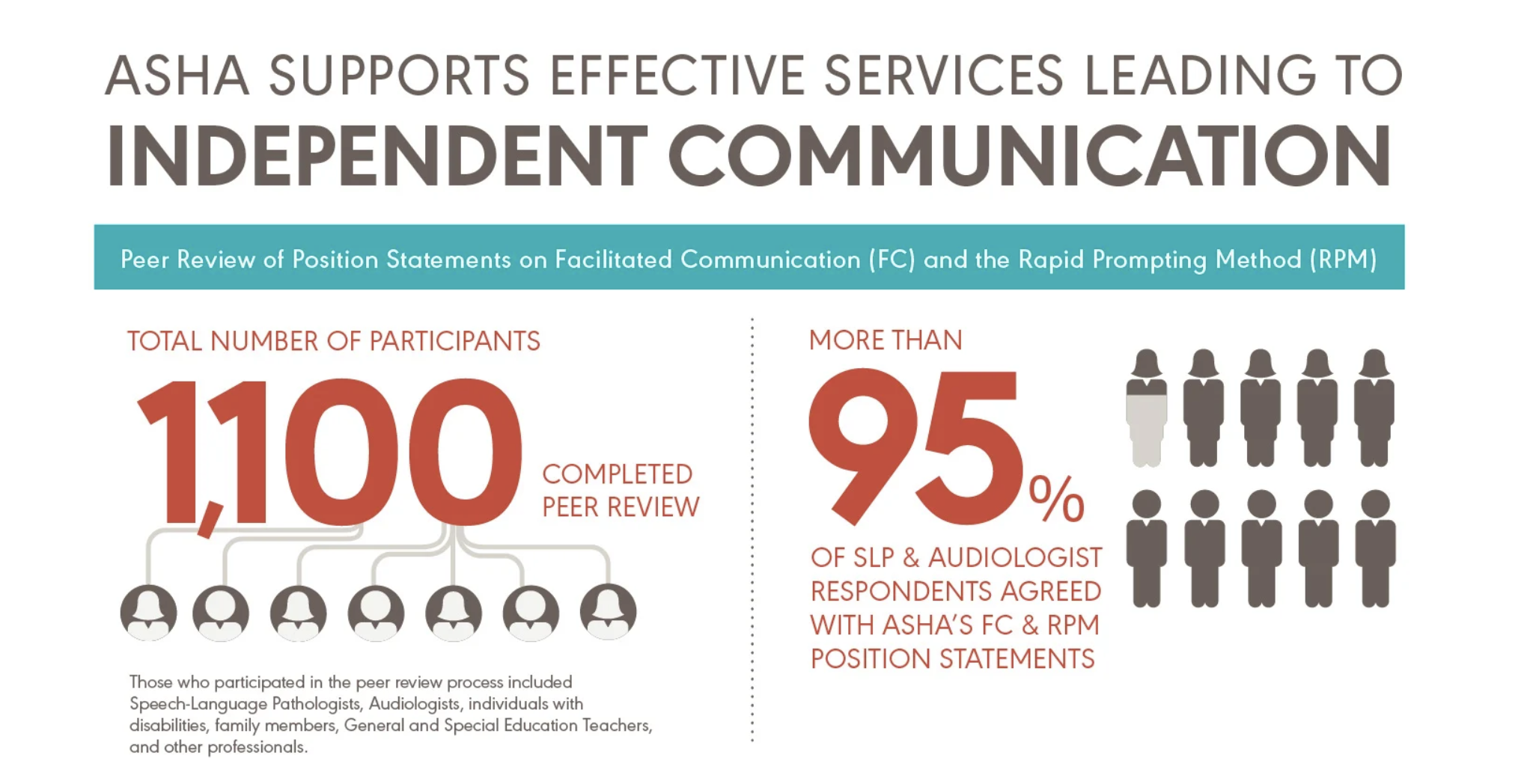
Image from the ASHA website (2018)
The goal of the Conlon, et al. study was to identify how confident and competent SLPs felt about assessing and treating individuals with complex communication needs using AAC and offer a way forward to further define and develop confidence and competence in SLP/AAC practitioners. The article sent me down a rabbit hole of reading similar studies which I’ll try to summarize in today’s blog post.
It shouldn’t be surprising to learn that the more training SLPs have, and the more specialized in AAC they are, the more confident they feel in treating individuals on their caseloads who would benefit from AAC to either supplement or replace their current communication systems. As I read these studies, two main points kept coming to mind:
(1) Assessing an individual for AAC and matching the person to the most appropriate system or systems of AAC isn’t as easy as it might appear to some, and
(2) general practice SLPs (those with limited training in AAC) or others outside the field might be more susceptible to adopting FC/S2C/RPM because these techniques seem to mimic low-tech forms of AAC and may seem easier to implement and less expensive than high-tech forms of AAC, which require funding and extensive training to use (although a recent study raises questions about the cost of RPM training and implementation).

From Wikimedia Commons: The main page of an AAC device layout for English Speakers.
While FC/S2C/RPM proponents push the idea of presuming competence in their clients, largely, in my opinion, to avoid testing for authorship, specialists in AAC start with a holistic approach to assessing an individual’s communication needs and preferences. The more precisely the specialist can identify the unique characteristics of the individual being assessed (speech/language abilities, motor skills, cognitive abilities, physical/positioning requirements, preferences, etc.), the more precisely those needs can be matched to low-tech and/or high-tech communication systems. The goal for AAC specialists is to assist the individual (by feature-matching communication systems and devices) in accessing a communication system that allows the optimal amount of independence and self-sufficiency. The amount of assistance and the type of systems used is different for each person. In addition, AAC specialists often offer their clients a range of options—to be trialed during the assessment period—so that selections can be made that best fit the individual in a variety of environments (e.g., home, school, store, recreation). There is no one-size-fits-all solution and, often, the AAC system used by the individual continues to evolve and change not only with use but with the abilities and needs of the client.
The more I read about this topic, the sadder I feel for FC/S2C/RPM proponents who reject the advice of SLPs in general, but particularly SLPs trained in AAC. I don’t doubt that some proponents have had frustrating experiences with SLPs and, perhaps gaining access to high-tech communication devices, but to me, that speaks to the need to provide appropriate support both to the families seeking help and to the SLPs who are tasked with assessing the speech and language needs of a broad spectrum of clients.
People (not just SLPs) who speak out against FC/S2C/RPM or call for reliably controlled testing of the techniques before adopting them are often portrayed by proponents as uncaring and ableist. But I’d argue that SLPs (whether they specialize in AAC or just have a foundational understanding of it) have their clients’ best interests at heart. I’d also argue that those who are least trained in the concepts of AAC are the most likely to adopt FC/S2C/RPM, perhaps bowing to pressure from parents or outside FC/S2C/RPM practitioners or to their own, internal pressures to provide an answer to a complex communication problem (often without fully understanding the problems of cueing and control over letter selection that occurs with facilitator-dependent techniques).
A common theme in the articles I read is that SLPs tend to make speech/language recommendations based on their own experience and education and/or familiarity with systems or technology. An SLP who was exposed to AAC in an introductory course during his or her training is going to make different suggestions than an SLP who later went on to specialize in AAC (through additional training and coursework).
The articles also suggested that SLPs with greater numbers of individuals on their caseloads requiring AAC felt more confident about their ability to assess and implement AAC treatment options. Other factors included work environment (schools, care facilities, hospitals), access to equipment and devices, access to other professionals for consultation services (AAC specialists, Occupational Therapists, Physical Therapists), and funding. This isn’t to say that general practice SLPs weren’t competent or caring about their clients, but SLPs specializing in AAC tended to consider a broader array of information when assessing the abilities, needs, and preferences of individuals requiring assistance. It seems a shame to reject their expertise.
In any event, as I read these articles, I jotted down some questions that might be useful for people seeking to assess, then implement an AAC system. I’m sure I’ve missed some, so please, if you think of any that should be added to the list, let me know.
Is there case history documentation that provides information about the individual’s motor ability, visual acuity, hearing, cognitive-linguistic abilities or challenges, medical history, etiology, etc.?
Has there been a complete language and communication assessment (e.g., receptive/expressive language, communication skills, communicative competence in a variety of settings)? Has the individual’s speech intelligibility been assessed (e.g., articulation, speech rate, tone)? To what extent will speech (e.g., articulation, verbal output) be part of the individual’s overall communication system? What are the individual’s speech and/or language abilities when aided and unaided?
What is the individual’s ability to identify and use symbols, to categorize those symbols, and navigate the organization system unique to a particular AAC system? What is the individual’s ability to understand and use written language (e.g., literacy skills, letter identification, spelling, understanding and use of the constructs of written language)?
How will the individual interact with the device or communication system (e.g., hand, finger, muscle movement, head mouse or eye tracking device)? Has there been an assessment of the individual’s gross and fine motor abilities? What is the optimal seating and/or positioning for the individual (both for comfort and protection of the person’s joints, as well as for accessing the device)?
Does the individual need a multi-modal approach to access a variety of low-or high-tech throughout the day and in different environments. Does, for example, the person need to be repositioned throughout the day from sitting to laying down? Does this change his/her ability to access the device(s)?
What feature(s) will the device have (e.g. portability, size of switches, alphabet/keyboard, speech-generating options)? Can these be adapted as an individual’s motor abilities change (e.g., in the case of individuals with ALS)?
Does the individual and his/her primary communication partner(s) understand why particular AAC systems were adopted or rejected? Do they understand how to navigate the system appropriately? Was there a trial period in which several AAC systems were tried and evaluated for effectiveness and appropriateness for the individual?
Will the AAC system supplement traditional speech/language treatments (e.g., development of verbal skills) and/or will the AAC system take the place of those treatments? How and why were these decisions made?
What procedures will be put in place to assess the effectiveness of the AAC system? Can the system be adapted to the individual’s wants, needs, daily activities, and preferences?
Is the AAC system being considered evidence-based? What are the pros and cons of the system (e.g, portability, access, organization of information, adaptability)? Is there funding available to assist the individual in accessing the treatment and equipment?
Recommended Reading:
Conlon, C., Zupan, B., & Preston, R. (2024). The confidence and competence of speech language pathologists in augmentative and alternative communication: a scoping review. Augmentative and Alternative Communication, 1–14. https://doi.org/10.1080/07434618.2024.2333383
Dietz, A., Quach, W., Lund, S.K., and McKelvey, M. (2012). AAC Assessment and Clinical-Decision Making: The Impact of Experience. Augmentative and Alternative Communication. 28 (3), 148-159. DOI: 10.3109/07434618.2012.704521.
Edelson, S. M., Rimland, B., Berger, C. L., & Billings, D. (1998). Evaluation of a mechanical hand-support for facilitated communication. Journal of Autism and Developmental Disorders, 28, 153-157. DOI: 10.1023/A:1026044716536
Hemsley, B., Bryant, L., Schlosser, R.W., Shane, H.C., Lang, R., Paul, D, Banajee, M., Ireland, M. (2018). Systematic review of facilitated communication 2014-2018 finds no new evidence that messages delivered using facilitated communication are authored by the person with disability. Autism and Developmental Language Impairments, 3, 1-8. DOI: 10.1177/2396941518821570
Lund, S.K., Quach W., Weissling, K., McKelvey, M., and Dietz, A. (2017, January). Assessment with Children who need Augmentative and Alternative Communication (AAC). Language, Speech, and Hearing Services in Schools. Vol. 48, 56-68.
McKelvey, M., Weissling, K.S.E., Lund, S.K., Quach, W. and Dietz, A. (2022). Augmentative and Alternative Communication Assessment in Adults with Amyotrophic Lateral Sclerosis: Results of Semi-Structured Interviews. Communication Disorders Quarterly. Vol. 43 (3), 163-171.
Scheibel, Gretchen, Zane, Thomas L., and Zimmerman, Kathleen N. (2022, January 20). An economic Evaluation of Emerging and Ineffective Interventions: Examining the Role of the Cost When Translating Research into Practice. Exceptional Children. https://doi.org/10.1177/00144029211073522
Schlosser, Ralf W. (2002, March). On the Importance of Being Ernest about Treatment Integrity. Augmentative and Alternative Communication. Vol. 18, 36-44,
Schlosser, R.W., Hemsley, B., Shane, H. et al. (2019). Rapid prompting method and autism spectrum disorder: Systematic review exposes lack of evidence. Review Journal of Autism and Developmental Disorders, 6, 403–412.
Schlosser, Ralf W. and Raghavendra, Parimala. Evidence-Based Practice in Augmentative and Alternative Communication. Augmentative and Alternative Communication. Vol. 20 (1), 1-21. DOI: 10.1080/07434610310001621083.
Theodorou, E. and Pampoulou, E. (2022). Investigating the Assessment Procedures for Children with Complex Communication Needs. Communication Disorders Quarterly. Vol. 43 (2), 105-118. DOI: 10.1177/152740/20960643
Watson, R.M. and Pennington, L. (2015, March-April). Assessment and management of the communication difficulties of children with cerebral palsy: a UK survey of SLT practice. International Journal of Language and Communication Disorders. Vol. 50 (2), 241-259.